Ever wonder what a day in the life of a digital historian looks like? Yesterday, I participated in the Day of Digital Humanities 2014 and blogged a bit over there throughout the day.
Author: Lisa Smith
Nominations for Giants’ Shoulders #70

Gottfried Kneller, Portrait of Hans Sloane (Source: Scientific Identity: Portraits from the Dibner Library of the History of Science and Technology, Smithsonian Libraries)
Sloane’s birthday is rapidly approaching and April 16 just happens to coincide with a well-known History of Science/Medicine/Technology blog carnival. To celebrate Sloane’s birthday this year, I’ll be hosting Giants’ Shoulders #70. Huzzah!
Please send in your blog post nominations by April 15 at the latest. You can send them directly to me at lisa dot smith AT usask dot ca or to Thony Christie the GS mastermind.
(And don’t be shy–please do nominate your own blog posts, too…)
9 April Update: Thony Christie’s call for Giants’ Shoulders nominations includes a short bio of Sloane!
Nursing Fathers, Slacking Dads and False Assumptions
Things I learned on the weekend… Slacker dads watch sports instead of read their children stories. They avoid housework and childcare as much as possible. They prefer work-life to domesticity. And above all, they look upon “Wet Wipe” daddies—those who are prepared with things like spare nappies and who concentrate on what their children are doing—with contempt. Or so claims Alex Bilmes, editor of Esquire, who shared his “Confessions of a slacker dad” in The Guardian. Bilmes wonders when being a good father became so complicated, concluding that “[t]he expectations of fathers have changed. More is demanded of us.” Righto. And off he went at speed, riding on his false assumptions about fatherhood in the past!

A father feeding his infant whilst the mother attends to domestic jobs and a small child plays with its food. Etching after A. van Ostade, 1648. Image Credit: Wellcome Library, London.
Joanne Bailey, author of the excellent Parenting in England 1760-1830, certainly has much to say on the complexities of fatherhood, identity and parent-child relationships. Being a dad was not, historically, exactly a walk in the park (with or without a Scandinavian buggy). As Bailey points out in one of her blog posts, Georgian fathers experienced (and were expected to experience) a profound range of postive and negative emotions.
In another post, she explains that Georgian society expected men as well as women to be emotional beings, resulting in an ideal that fathers should be “tender” or “nursing” or—to use a modern term–“involved”. Victorian and mid-twentieth century fatherhood, by contrast, emphasised less emotional expression (particularly in men), shifting the cultural focus to fathers’ roles as breadwinners.
The anti-Wet Wipe father Bilmes would, I expect, be surprised by (what I now call) the Medicinal Plaister Papas of the early eighteenth century: the men who performed a wide range of caregiving roles within the household, including nursing and remedy preparation. The Sloane Correspondence is filled with concerned fathers who oversaw the health care of their children.
Many fathers provided detailed reports of their children’s health and administered treatments. In a letter dated 1 February 1697, John Ray grieved for his daughter who had died of an apoplectic fit after three days of delirium. He blamed himself for giving her one of his own remedies, only to see it fail on this crucial occasion.
William Derham was concerned about his “little daughter”, aged nine, on 3 November 1710. She had been “seized immediately with a great suffocation like to have carried her off divers times”. Derham reported his daughter’s symptoms (sore throat and lungs, heart palpitations and blindness) and described her treatments, including the use of a microscope to examine her eyes. It is possible that a local physician had undertaken the microscopic examination, as the language is ambiguous. But knowing Derham’s scientific interests, it seems more likely that Derham examined his daughter’s eyes himself.
Others were concerned that their own sins might be visited upon their offspring with terrible consequences. Edward Davies, on 8 July 1728, was worried that his son’s joint pain might affect his head. In addition to reading up on John Colbatch’s remedy for convulsive distempters ( A Dissertation Concerning Mistletoe, 1723), Davies had treated his son with Daffy’s Elixir. Davies had two main questions. First, he wondered if his own past mercury treatments (for venereal disease?) had caused his son’s ill health: “my blood was poyson’d in my youth with a Quicksilver-gird & I wish my off-spring do not suffer that”. Second, he was also unsure whether teaching his son Latin to prepare him for public school would do him more harm than good in his condition. Raising a child was a fraught venture, from passing on one’s own health problems to training them well for the future. In any case, Davies was deeply involved in his son’s upbringing.
Fathers also exchanged useful medical knowledge. In August 1723, Mr. Townshend wrote to Sloane that his daughter Ann had been on her way to visit Sloane about her blindness, but Townshend had such trouble parting with her that she would be “14 days longer”—and he would have preferred it if Sloane could come to Exeter! A month later, Townshend expressed his gratitude for Sloane’s help, although Ann was no better. Townshend had, nonetheless, suggested that Mr. Farrington and others contact Sloane for assistance.
Sure enough, that same day, Mr. Farrington had written to Sloane about his daughter’s eye problems. Farrington noted that when his daughter (now 21) was ten, she’d suffered from such violent head pain that she was expected to die. She eventually lost sight in both her eyes and although she was able to move around the home and gardens, she was unable to travel beyond them. Farrington described the nature of her limited sight, as well as the treatments and diagnosis that she had received. By the next month, Farrington waivered between hope and despair based on Sloane’s (unknown) response, but he sent Lady Yonge to collect Sloane’s remedies. As of 23 November 1723, Farrington noted that Sloane’s treatments seemed to be working “and the load she hath had above the eyes taken off”.
These last two cases reveal two worried fathers, both of whom were familiar with the details of their daughters’ treatments. Townshend’s recommendation of Sloane’s assistance to his friends also suggests a network of fathers who exchanged medical knowledge—in the case of Townshend and Farrington, about their daughters’ shared problem.
Distant dads? Not at all! These early eighteenth-century Medicinal Plaister Papas who wrote to Sloane had far more in common with the modern Wet Wipe fathers than Bilmes and his Slacker Dad ilk.
An Eighteenth-Century Case of Cotard Delusion?
Recently, I found myself doing a little seat dance in the British Library when I came across a fascinating series of letters (Sloane MS 4076) from 1715, written by apothecary William Lilly about the Countess of Suffolk, Henrietta Howard. Historians of medicine, of course, are generally loathe to engage in retrodiagnosis, but sometimes it’s just too tempting… What Lilly seemed to be describing was a case of Cotard Delusion!
Cotard Delusion, or Walking Corpse Syndrome, was first described as a cluster of symptoms by Jules Cotard in the 1880s. The symptoms include insensitivity to physical pain, a preoccupation with guilt and despair, and the belief that one is already dead, damned or possessed (or, conversely, immortal). Cotard was not the first to observe this sort of case, but he categorised it as a syndrome: hypochrondriac delusion and anxious melancholy, or lypemania—drawing on an earlier classification from Jean-Étienne Dominique Esquirol (1772-1840).

The corpse of a lady wearing a ruff and an elaborate head-dress.
Credit: Wellcome Library, London.
According to modern studies, Cotard Delusion starts off with a sense of general anxiety that could last weeks or years, but increases over time until the patient believes s/he is dead and is preoccupied with guilt and despair. Sometimes this is accompanied by muteness or paralysis. In some cases, the disorder might be accompanied by physical problems, such as a brain tumour or injury, multiple sclerosis, or Parkinson’s disease.
So what were Lady Suffolk’s symptoms? In a letter dated 20 July (ff. 7-8), Lilly noted that Lady Suffolk was taking little rest, but
“when she waked from her slumber call’d out in a frightfull manner for half an hour that she was deceased and a great deal of such Language”.
Once this “raveing fitt” ended, she became profoundly drowsy and “lay still without any motion”. She needed help with the bedpan, even “though she walk’d severall turns in her Bed Chamber yesterday”. Lilly bled her nine or ten ounces, which he hoped would prevent worse lethargy. Lady Suffolk’s blood was viscous and sizy. Lilly thought it suggested, along with her stopped urine, a “phrenites [acute inflammation of the mind and body] with the Mania”. Lilly also applied blisters on her legs to draw the bad humour down and out, laid pigeons to her feet (sometimes used to treat headaches and migraines) and shaved her head to relieve the excess heat in the head.
Four days later, Lilly had administered Sloane’s prescriptions “without the desired effect” (f. 9). Lady Suffolk no longer had a fever, but her other symptoms continued and she was drowsy, “which made me fear her turning lethargical or some other distemper on her Braine which I perceved to be already affected”. Lilly gave Lady Suffolk a glister, inducing her to flow in several ways. She produced a large stool and plenty of urine and spoke more than she had in two days.
On 26 July, Lilly reported that Lady Suffolk had vomited phlegm and choler, as well as had three stools. She could walk around her chamber, but “still continues very melancholy and silent and seldom speaks without being importuned to it”. Lilly was deeply worried. He hoped that Lord Suffolk would take his wife to London “where you may see her oftener”, as her “present indisposition will not quickly be removed”. Lilly again suggested that it might be an affectio hypochondrica [melancholy] or mania, and provided details about Lady Suffolk’s conversation:
“for what she sayes is that she is undone in soul and body that she is sure she will be damned at other times when I urge her to speaks she tells me she is dead and has been so for some time”.

After M. de Vos, A woman beleaguered by demons, death and deceiving angels; representing faith resisting the evils of the world. Source: Wellcome Library, London.
In an undated letter that seems to come at this point in the series (ff. 12-13), Lilly listed Lady Suffolk’s symptoms as diarrhoea, fever and head pain and insisted again that the disorder was hysterical, not feverish. Given Lilly’s repeated attempts to persuade Sloane that the real problem was hysterical, it’s not clear that Sloane initially trusted Lilly’s diagnosis.
But by late July, Sloane had started prescribing anti-hysterical medications, including cordials and drops (29 July, ff. 10-11). Even so, Lady Suffolk “is more than usually melancholy” and complained of heart palpitations and swimming in the head: more symptoms of hysteria. Since Lady Suffolk’s fever had not returned, Lilly hoped that the danger had passed.
This sort of delusion was distressing to observers, including Lilly who was uncertain of his ability to help, but Lady Suffolk’s disorder was readily classified as hysteria or hypochondria—ailments that were as much physical as mental. The diagnosis and treatment for Lady Suffolk was humoral in nature, treating her emotions as fluids and using remedies to make her body and mind flow.
Although retrodiagnosis is tempting in Lady Suffolk’s case, eighteenth-century medicine already had a place for her religious delusions. Robert Burton, for example, included a lengthy section on religious melancholy in his famous Anatomy of Melancholy (1621). Eighteenth-century books on hypochondria also emphasised the often religious nature of sufferers’ fears, such as despair and damnation, especially in women (e.g. Nicholas Robinson, A New System of the Spleen, Vapours, and Hypochondriack Melancholy, 1729).
Retrodiagnosis is unhelpful in another way. Lady Suffolk was ill with problems besides the delusion, which had even lessened toward the end. In particular, Lady Suffolk’s ailments progressed rapidly in less than a month.
Lady Suffolk never made it to London to see Sloane in person. The danger had not passed: she died on the 10th of August.
References
G.E. Berrios & R. Luque, “Cotard’s Delusion or Syndrome?: A Conceptual History”, Comprehensive Psychiatry 36, 3 (1995): 218-223.
Hans Debuyne, Michale Portzky, Frédérique Van den Eynde, Kurt Audenaert, “Cotard’s Syndrome: A Review”, Current Psychiatry Reports 11, 3 (2009): 197-202.
An Eighteenth-Century Love Story
The Newdigate family became Hans Sloane’s patients around 1701, starting with Lady Frances Sedley (née Newdigate), her husband, and father-in-law. By 1705-6, Sloane was treating Elizabeth Newdigate (b. 1682) for colic, hysteria and fever (BL Sl. MS 4076, 1 July 1705, f. 173; 4077, 21 December 1706, f. 164). But Elizabeth’s complaints went far beyond the medical.
A letter of 1 November 1706 detailed her illness, penury, and unhappy family situation. Specifically, she blamed the “distruction of my health if not to the loss of life” on her brother and sisters who were “miserably unkind” to her. This was partly financial, as her brother Dick
wou’d not help me to one peny of money when I was sick in London but forsed me to borow of strangers.
Dick had apparently even written to “all my Relations [that] I unjustly demanded mony of him when he was not in my debt”.
But the siblings were being unreasonable in another way, too. They had dismissed her illness, telling everyone “that I was distracted and had no illness but that of being in love”. She swore innocence in the matter, insisting that she had not even really spoken to the man.

Theodore Lane, A young woman escapes down a rope of sheets, intending to elope with her lover, n.d. Credit: Wellcome Library, London.
Of course, she must have done… or perhaps her siblings had put the idea of an unsuitable match into head. A year later, she married Abraham Meure, the son of a Huguenot schoolmaster–self-styled a “Gent.” in the marriage contract of 3 September 1707 (Warwickshire County Record Office, CR 136 C2734).
For a woman from a good gentry family, this was a bad choice of husband. A torn-out page from the family Bible makes clear that Elizabeth had “married herself” (WCRO, CR 136/B830). Her father made the point again in the marriage settlement, promising “That for and notwithstanding the consent and good likeing of the said Sr Richard Newdigate is not obtained”, he would still pay her portion. Abraham, nonetheless, does appear to have been a man of some means. Not only did he renounce his claim on and interest in Elizabeth’s portion, “out of the great love and affection” he had for her, but he would provide an annuity of £300.
Elizabeth’s letter reads like a cry for pity. Perhaps, by playing upon her defenselessness, she hoped to persuade Sloane to mediate on her behalf. Given her eventual success in marrying Abraham, it is entirely possible that Sloane did help. Sloane certainly continued on as physician to the Newdigate and Meure families. And over time, Abraham became a close member of the family, helping his brother-in-law William Stephens during financial difficulties.
Unfortunately, Elizabeth and Abraham’s match was short-lived. Elizabeth died on 9 July 1710, just two weeks after giving birth to their son John.
The Problem of Mad Dogs in the Eighteenth Century
Surgeon John Burnet shared “a very strange account” with Sir Hans Sloane in March 1720. The tale, sent to the French Académie des Sciences, had come straight from the Czar of Muscovy (Peter the Great) himself. Apparently,
a Man was bitt by a Mad-dog & that he lay with his wife the same night & after three fitts dyed, but that his wife was brought to bed nine weeks afterwards of five puppies.
Curious, indeed. Did this mean that rabies (or hydrophobia, as it was called) might be spread like a venereal disease? Or that the dog-bite had transmitted canine qualities into the infected man, which he then passed on to his offspring? Burnet was sceptical about account, noting “how far this is true, I know not”, but similar stories could be found in the Philosophical Transactions.
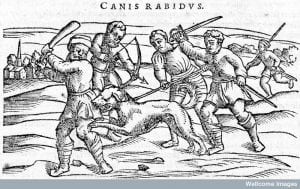
Rabies: Slaying a mad dog. From Dioscordes, Acera de la materia medicinal y de los venenos, 1556. Credit: Wellcome Library, London.
Physician Martin Lister, for example, wrote “An Observation of Two Boys Bit by a Mad Dog” (1698). Back in 1679, two boys aged nine and ten washed the head wounds of a dog that had been bitten by a mad dog. The injured dog was saved, but several months later, the boys became ill with stomach pains and convulsions.
What suggested a diagnosis of hydrophobia was that, by August 1680, the boys feared the water and had become, well, a bit dog-like. They regularly went into simultaneous fits that would last an hour, during which time “the Eldest especially, snarled, barked and endeavoured to bite like a Dog”. By September, “they became more wild” and, even after the fits had passed, could not endure the company of people. They had become more animal than human. The case seemed dire, but the boys were on the mend by the end of September.
Clergyman and antiquary, Abraham de la Pryme, wrote to Sloane in 1702 about a 1695 case from his brother’s household (see also Phil. Trans. 23, 1702-3). De la Pryme noted the regularity of timing in several cases, but was particularly intrigued by the way that tiny “Particles of this Poyson” could spread to infect a “mass of particles millions of times bigger”.
This case started with a “pretty grey-hound Bitch that had Whelps” being bitten by a mad dog. Three weeks later, the greyhound also went mad and had to be put down. The puppies appeared well and were looked after, but (again) three weeks later, “all pull’d out one anothers throats except one”. This one continued to eat, but would drink no liquid. Two servants caring for the puppy stuck their fingers into its mouth to check for a blockage, but there was none. The puppy soon went mad.
Three weeks later, both servants became ill. One, “a most strong and laborious Man”, managed to sweat off his symptoms: acute headache, tightened throat and red eyes (which makes me think of Black Shuck’s fiery eyes). But the fourteen-year old apprentice was much sicker. He became so savage that it took four adult men to hold him down
and all his discourse was of fighting, and how if that they would but let him alone, he would leap upon them, and bite, and tear them to pieces.
He soon lost his ability to speak altogether (one of the marks of humanity), then died.
The economic problem of the disease was obvious, as it could easily spread to livestock. In George Dampier’s recipe for rabies (published in the Phil. Trans.), Dampier reported that his remedy “did [his neighbours] a Hundred Pound’s Worth of Good” during a local outbreak when it saved their cattle.
But the social consequences of transmission was even more worrying. Rabies was, after all, considered a type of poison (see here and here), but so too was venereal disease, which could also be passed to one’s offspring. The real fear? That the mad animal’s qualities might be passed on to the human—or, worse yet, the victim’s children.
As De la Pryme concluded in his account, it was a pity “that the most Noble of creatures lyes at the Mercy of the most ignoble of particles”, but a wonder “that a few Atoms should be able to destroy a whole world”.
The Preserved Puppy Proposal
Edmund Curll, a bookseller’s apprentice, wrote to Sloane in 1703 with news of “A Wonderfull production in Nature”: an unusual puppy.
Recently, a Scottish gentleman’s dog had
Whelp’d two Puppies one of them was whelp’d dead and the other that was whelp’d alive being a Male in 24 hours after voided from the fundament another Little Creature wch Liv’d 10 Hours and is now preserv’d in Spirits of Wine.
This, Curll promised Sloane, could “be produced Sr if you please to give yourself the trouble”.

Experiment on a dog. From Joannes Walaeus, Epistola duae, 1651. Credit: Wellcome Library, London.
By 1703, Sloane was already known for his collection of curiosities, but it was in Sloane’s capacity was secretary of the Royal Society that Curll approached him (as the letter’s address specified). Presumably Curll thought that Sloane, in particular, would be unable to resist a strange “Little Creature” born from its mother’s anus.
Dogs, of course, were often used in experimentation, so an unusual specimen may well have been of interest to the Royal Society—though I would have been more curious to examine the mother to determine whether the anal birth had resulted from a congenital problem or an injury caused by the whelping.*
In writing to Sloane, perhaps Curll was hoping to strike up a common interest with a potential patron who was known for buying books as well as oddities—or, maybe, he was just hoping to turn a quick profit on a dead puppy.
Capitalizing on (bad) luck and death was certainly one of Curll’s overall career-building tactics. In 1708, he took over his master’s bookselling after Roger Smith went bankrupt. And his career went from high to high (or low to low), as Curll became infamous as a seller of dodgy remedies to treat venereal problems and a purveyor of cheap dirty books and scandals. He was also known for publishing scurrilous and unverified biographies of recently deceased people, leading physician John Arbuthnot to (allegedly) comment that Curll was “one of the new terrors of death”.
Was it a coincidence that Curll can be spotted trying to sell Sloane a preserved puppy so early in his bookselling life? Or was the puppy a harbinger of Curll’s future approach to his career?
* My internet search history is now filled with some pretty iffy search terms and I’m no wiser, although I suspect an injury. I also discovered that there are a lot of preserved puppies available for sale on ebay and etsy, but no relevant historical pictures of such specimens.
Recording Dr. Sloane’s Medical Advice
Sir Hans Sloane might have collected recipe books in search of knowledge, but patients in turn might record his medical advice for later reference. The Arscott Family’s book of “Physical Receipts”, c. 1730-1776 (Wellcome Library, London, MS 981), for example, contains three recipes attributed to Sloane, which provides snippets of information about his medical practice.
Although Sloane was best known for his botanical expertise and promotion of treatments such as Peruvian Bark or chocolate, the Arscott family recipes show a mixture of chemical, animal and herbal remedies. The treatment for worms (f. 129), for example, combined a mixture of elixir proprietatis and spirit. salis dulcis in either white wine or tea. Together, these aimed to sweeten the blood, strengthen the nerves and fortify the stomach.
![A woman is carrying a tray with a cup of chocolate [or maybe the pleurisy remedy?] and a glass on it. Credit: Wellcome Library, London.](http://sloaneletters.com/wp-content/uploads/2014/01/Cup-of-chocolate.jpg)
A woman is carrying a tray with a cup of chocolate [or maybe the pleurisy remedy?] and a glass on it. Credit: Wellcome Library, London.
The pleurisy remedy (f. 156) included pennyroyal water, white wine and “2 small Balls of a sound stone horse”—or, dung from a horse that still had its testicles. This was to be steeped for an hour, then strained. (Apparently this weakened the taste of the dung.) This delicious liquor would keep for three days. Are you tempted? Because the dose was a “large Chocolate Dish fasting in the morning and at 4 in the Afternoon”. “If the Stomach will bear it” (and whose wouldn’t?), the patient was to take the remedy for four to six days in a row. In this remedy, the dung was the most powerful ingredient, as it was considered a sudorific (causing sweat) and resolvent (reducing inflammation) that would aid asthma, colic, inflamed lungs, and pleurisies.
Sloane, of course, was also famed for his eye remedy, which he made public knowledge in 1745 when he published An Account of a most efficacious medicine for soreness, weakness, and several other distempers of the eyes. But how close to the published remedy was the Arscott version? Fortunately, the most detailed of the three recipes is “Sr Hans Sloane’s Direction for my Aunt Walroud in ye Year 1730–when she perceiv’d a Cataract growing in one of her Eyes” (ff.79-80).

Sloane’s remedy would have been preferable to being couched for a cataract. Heister, Operation for cataract and eye instruments, 1757. Credit: Wellcome Library, London.
Although there are measurements and preparation details, just like a recipe, it was also a summary of Sloane’s successful medical advice to Mrs Walroud. Of course, what early modern patients deemed success in a treatment differs from our modern concept. For Mrs Walroud, it was enough that after she started the treatment at the age of 67, her eyes did not get any worse for ten years and “she could write & read tolerably well”. When she died at the age of 83, she still had some of her sight.
The Arscott instructions begin by recommending that the sufferer have nine ounces of blood taken from the arm and a blister applied behind the ears. Next, take a conserve of rosemary flowers, pulvis ad guttetam (ground human skull mixed with various herbs), eyebright, millipedes, fennel seed and peony syrup. Last, the patient was to drink a julap (medicine mixed with alcohol) of black cherry water, fennel water, compound peony water, compound spirit of lavender, sal volat oleos and sugar. Mrs Walroud took both twice daily and kept a “perpetual Blister between her shoulders”.
One crucial difference between Sloane’s published remedy and the Arscott one is that no mention is made in Mrs Walroud’s treatment of using an ointment made of tutty (oxide of zinc), lapis haematites, aloes, prepared pearl and viper’s grease. Three possibilities for the ointment’s absence occur to me.
- The Arscott family may have simply assumed that the listed directions were intended to accompany the purchase of Sloane’s ointment and didn’t specify something so obvious.
- The reference to using the ointment was lost when the instructions had been passed between family members.
- Or, Sloane did not always prescribe the ointment.
The remaining directions, though, do have overlaps. In his Account, Sloane prescribed drinking a medicine that also contained rosemary flowers, pulvis ad guttetam and eyebright—though he included more ingredients: betony, sage, wild valerian root and castor. This was to be followed by a tea (rather than julap) with drops of compound spirit of lavender and sal volat oleos. In this case, it was the Arscott version that included extra ingredients.
The type of bleeding in the Account was also slightly different than Mrs Walroud’s, with the recommendation that six ounces of blood be taken either from the temples using leeches or by cupping at the shoulders. Sloane’s eye remedy was supposed to be useful for many types of problems, he did not prescribe it exactly the same each time. Variations were possible, according to the patient and the problem.
The Arscott recipes suggest not only what advice from Sloane the family had found most useful, but what sorts of remedies Sloane might prescribe to his patients. But whatever Mrs Walroud’s rave review, the next time I suffer from eye strain at the computer, I won’t be reaching for Sloane’s drink with pulvis ad guttetam and millipedes in a hurry.
Sloane Family Recipes
In his Recipes Project post, Arnold Hunt focused on the recipe books owned by Sir Hans Sloane. The Sloane family may have had an illustrious physician and collector in their midst, but they, too, collected medical recipes like many other eighteenth-century families. As Alun Withey points out, medical knowledge was of part of social currency. Three Sloane-related recipe books that I’ve located so far provide insight into some of the family’s domestic medical practices and interests.
Elizabeth Fuller: Collection of cookery and medical receipts
Credit: Wellcome Collection, London.
Two books are held at the British Library, donated in 1875 by the Earl of Cadogan. A book of household recipes, primarily for cookery, was owned by Elizabeth Sloane—Sloane’s daughter who married into the Cadogan family in 1717 (BL Add. MS 29739). The second book, c. 1750, contained medical, household and veterinary recipes (BL Add. MS 29740), including several attributed to Sir Hans Sloane. A third book, which belonged to Elizabeth Fuller, is held at the Wellcome Library (MS 2450) and is dated 1712 and 1820. Given the initial date and name, it is likely that the book’s first owner was Sloane’s step-daughter from Jamaica, Elizabeth Rose, who married John Fuller in 1703. Sloane’s nephew, William, married into the Fuller family as well in 1733.
Elizabeth Sloane, of course, compiled her collection long before her marriage; born in 1695, she was sixteen when she signed and dated the book on October 15, 1711. This was a common practice for young women who were learning useful housewifery skills. The handwriting in the book is particularly good, with lots of blank space left for new recipes, suggesting that this was a good copy book rather than one for testing recipes. There are, even so, some indications of use: a black ‘x’ beside recipes such as “to candy cowslips or flowers or greens” (f. 59), “for burnt almonds” (f. 57v) or “ice cream” (f. 56). The ‘x’ was a positive sign, as compilers tended to cross out recipes deemed useless.
The Cadogan family’s book of medicinal remedies appears to have been intended as a good copy, but became a working copy. In particular, the recipes to Sloane are written in the clearest hand in the text and appear to have been written first. Although there are several blank folios, there are also multiple hands, suggesting long term use. There are no textual indications of use, but several recipes on paper have been inserted into the text: useful enough to try, but not proven sufficiently to write in the book. As Elaine Leong argues, recipes were often circulated on bits of paper and stuck into recipe books for later, but entering a recipe into the family book solidified its importance—and that of the recipe donor—to the family.
Sloane’s recipes are the focal point of the Cadogan medical collection. Many of his remedies are homely, intended for a family’s everyday problems: shortness of breath, itch, jaundice, chin-cough, loose bowels, measles and worms. There are, however, two that spoke to his well-known expertise: a decoction of the [peruvian] bark (f. 8v)—something he often prescribed–and “directions for ye management of patients in the small-pox” (f. 10v).
Elizabeth Fuller compiled her book of medicinal and cookery recipes several years after her marriage and the book continued to be used by the family well into the nineteenth century. The book is written mostly in one hand, but there are several later additions, comments and changes in other hands. The recipes are idiosyncractic and reflect the family’s particular interests: occasionally surprising ailments (such as leprosy) and a disproportionate number of remedies for stomach problems (flux, biliousness, and bowels). The family’s Jamaican connections also emerge with, for example, a West Indies remedy for gripes in horses (f. 23). There are no remedies included from Sloane, but several from other physicians.
This group of recipe books connected to the Sloane Family all show indications of use and, in particular, the Cadogan medical recipe collection and the Fuller book suggest that they were used by the family over a long period of time. Not surprisingly, the Fuller family drew some of their knowledge from their social and intellectual networks abroad.
But it is the presence or absence of Sloane’s remedies in the books that is most intriguing. Did this reflect a distant relationship between Sloane and his step-daughter? Hard to say, but it’s worth noting that his other step-daughter, Anne Isted, consulted him for medical problems and the Fuller family wrote to him about curiosities.
Or, perhaps, it highlights the emotional significance of collecting recipes discussed by Montserrat Cabré. Sloane was ninety-years old when the Cadogan family compiled their medical collection.

Hans Sloane Memorial Inscription, Chelsea, London. Credit: Alethe, Wikimedia Commons, 2009.
It must have been a bittersweet moment as Elizabeth Cadogan (presumably) selected what recipes would help her family to remember her father after he died: not just his most treasured and useful remedies, but ones that evoked memories of family illnesses and recoveries.
Recipes in Sir Hans Sloane’s Collections
Happy New Year!
This week, I have a couple recipes-related posts planned in response to Arnold Hunt’s fascinating interview at The Recipes Project on recipe books from Sloane’s collection. Hunt, a Curator of Manuscripts at the British Library (and friend of this blog), has much to say on the process of collecting and curating, as well as recipe books.
You should read it.